CLINICAL WORKFLOW INTEGRITY™
The Alignment of Clinical Intent, Workflow, and Interface in Healthcare Delivery
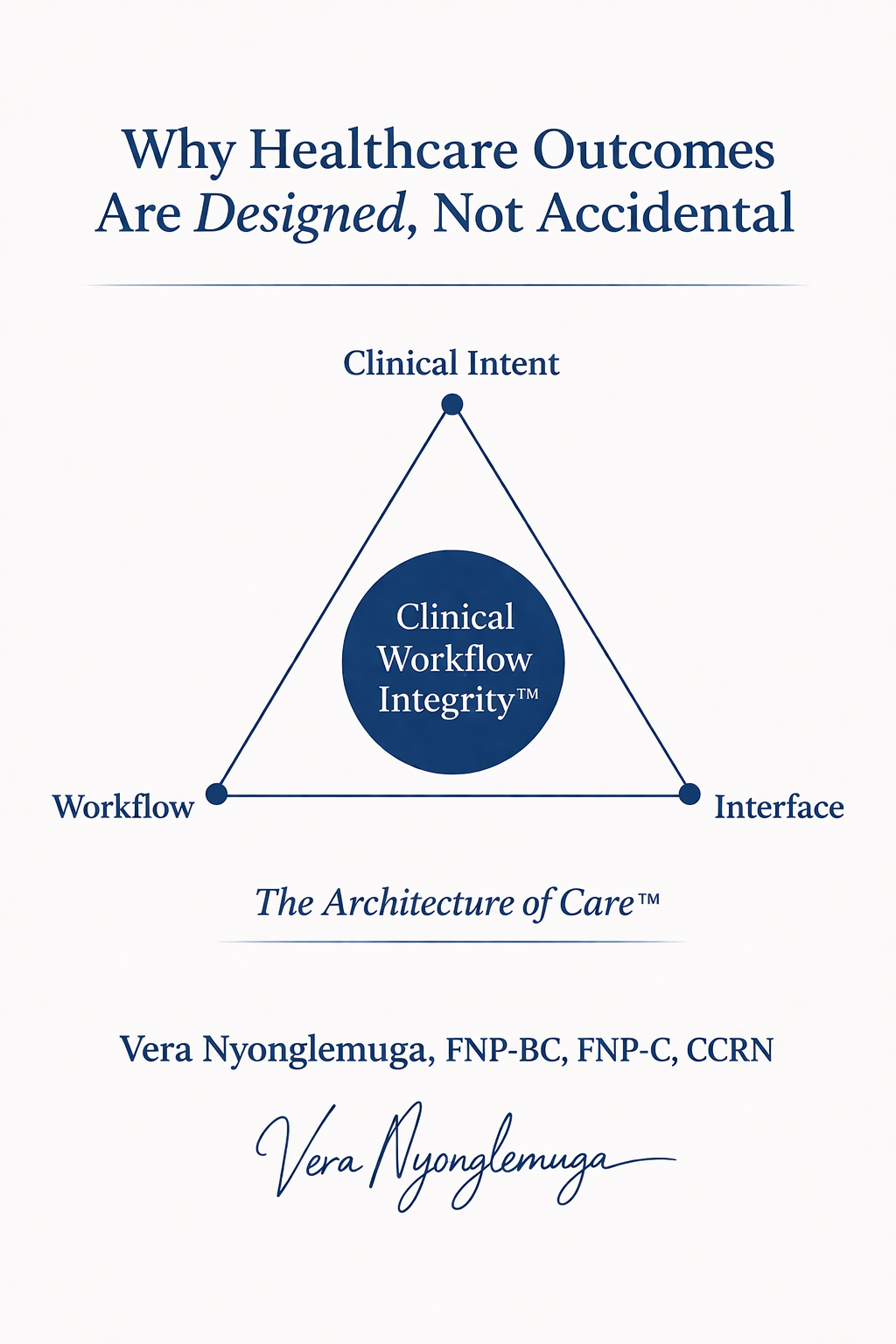
Healthcare systems are defined not only by what they intend to deliver-but by how clinical intent, workflow, and interface align.
Clinical care does not fail solely because of gaps in knowledge, effort, or resources.
It fails when the structure through which care is delivered does not support how clinical decisions are meant to be made.
Clinical Workflow Integrity™ describes the degree to which clinical intent, workflow, and the healthcare interface are aligned.
This alignment determines whether care is continuous or fragmented, whether decisions are informed or reactive, and whether outcomes are achievable or theoretical.
The Core Misalignment Problem
In many healthcare systems, the components of care exist—but they do not function together.
Clinical intent is defined by evidence, training, and best practice
Workflows are shaped by scheduling, operational constraints, and throughput demands
Interfaces are determined by EHRs, communication tools, and access structures
When these components are misaligned, clinicians are forced to operate within systems that do not support the care they are trying to deliver.
The result is predictable:
Clinical reasoning is interrupted or incomplete
Important information is unavailable at the point of decision-making
Care plans are not carried forward across encounters
Follow-up becomes reactive rather than structured
These are not isolated operational failures.
They are failures of alignment.
The Clinical Workflow Integrity™ Model
Clinical Workflow Integrity™ is built on three core elements:
1. Clinical Intent
What care is meant to achieve.
Clinical intent is grounded in:
diagnosis
prevention
longitudinal management
evidence-based decision-making
It reflects how clinicians are trained to think and what optimal care requires over time.
However, clinical intent alone does not determine outcomes.
It must be supported by the systems through which care is delivered.
2. Workflow
How care is actually delivered in practice.
Workflow includes:
scheduling structures
visit duration and format
follow-up processes
continuity planning
Workflow determines whether clinical intent can be executed.
When workflow is misaligned:
time is insufficient for complexity
follow-up is inconsistent
continuity is disrupted
Even strong clinical reasoning cannot overcome poorly designed workflow.
3. Interface
How clinicians and patients interact with the system.
The interface includes:
electronic health records (EHRs)
communication platforms
patient portals
access points to care
The interface determines:
what information is visible
how easily it can be accessed
whether it supports or obstructs decision-making
When the interface is misaligned:
critical information is fragmented or lost
clinicians rely on incomplete data
patients experience discontinuity and repetition
Alignment vs. Misalignment
Clinical Workflow Integrity™ is not defined by the presence of these components—but by their alignment.
When Alignment Is Absent
Clinical intent is disconnected from workflow constraints
Workflow does not support continuity or follow-up
Interfaces fail to deliver relevant information at the point of care
Care becomes:
episodic rather than longitudinal
reactive rather than proactive
fragmented rather than integrated
Outcomes become inconsistent and dependent on individual effort rather than system design.
When Alignment Is Designed
Workflow supports the execution of clinical intent
Time and scheduling reflect clinical complexity
Information flows across encounters and informs decisions
Interfaces reinforce continuity rather than disrupt it
Care becomes:
structured and continuous
anticipatory rather than reactive
grounded in complete clinical context
Outcomes improve—not through increased effort alone, but through alignment.
The Role of Clinical Workflow Integrity™ Within the Architecture of Care™
Clinical Workflow Integrity™ sits at the center of The Architecture of Care™.
While the broader architecture defines the structural environment of care,
Clinical Workflow Integrity™ determines whether that structure functions cohesively in practice.
Without alignment:
structural components operate in isolation
fragmentation persists
With alignment:
the system functions as intended
continuity becomes possible
outcomes become reproducible
What Changes in Practice
When Clinical Workflow Integrity™ is present:
Clinical decisions are made with complete and accessible context
Follow-up is intentional, structured, and expected
Care plans persist across encounters
Patterns are recognized earlier
Responsibility is clear and continuous
The experience of care changes for both clinicians and patients.
Clinicians operate within systems that support their reasoning.
Patients experience care as connected rather than fragmented.
Implications for Healthcare Systems
Improving healthcare outcomes is not solely a matter of increasing resources or effort.
It requires aligning the structures through which care is delivered.
Clinical Workflow Integrity™ provides a way to evaluate and redesign care delivery by asking:
Does workflow support clinical intent?
Does the interface support decision-making?
Does information persist across encounters?
Is continuity structurally enabled or left to chance?
These questions shift the focus from individual performance to system design.
Clinical excellence requires more than knowledge.
It requires systems that allow that knowledge to be applied consistently over time.
Clinical Workflow Integrity™ is the difference between care that is possible—and care that is reliably delivered.
Healthcare outcomes are not accidental.
They depend on alignment.
Alignment is not theoretical.
It determines how care is actually delivered.
→ See how this work is applied in real-world systems:
For Clinicians & Systems