

Why Am I So Angry Before My Period?

The Hidden Link Between Perimenopause, Mood Changes, and Hormones
Many women enter their late 30s and 40s feeling like they no longer recognize themselves.
They become irritated by things that never used to bother them.
Small frustrations suddenly feel overwhelming.
Patience becomes harder to find.
A minor inconvenience can trigger an emotional reaction that feels completely out of proportion.
Some women find themselves snapping at their partners, children, coworkers, or friends, only to feel guilty moments later.
Others describe feeling emotionally exhausted, unusually reactive, or as though they have become "a different person" for several days each month.
For many, these changes seem to occur most intensely in the days leading up to their menstrual period.
Naturally, many women begin asking themselves difficult questions.
"Am I becoming an angry person?"
"Why can't I control my emotions the way I used to?"
"Is something wrong with my mental health?"
"Is this simply stress, or could it be my hormones?"
"Why does this seem to happen every month?"
These concerns are incredibly common.
Yet they are also frequently misunderstood.
Many women blame themselves for these emotional changes, believing they are becoming overly emotional, impatient, or difficult to be around.
Others are told that it is "just stress," "just PMS," or simply a normal part of getting older.
While stress, life circumstances, and mental health certainly influence emotional well-being, they do not tell the entire story.
For many women, the answer lies within the remarkable biologic changes occurring during the menopause transition.
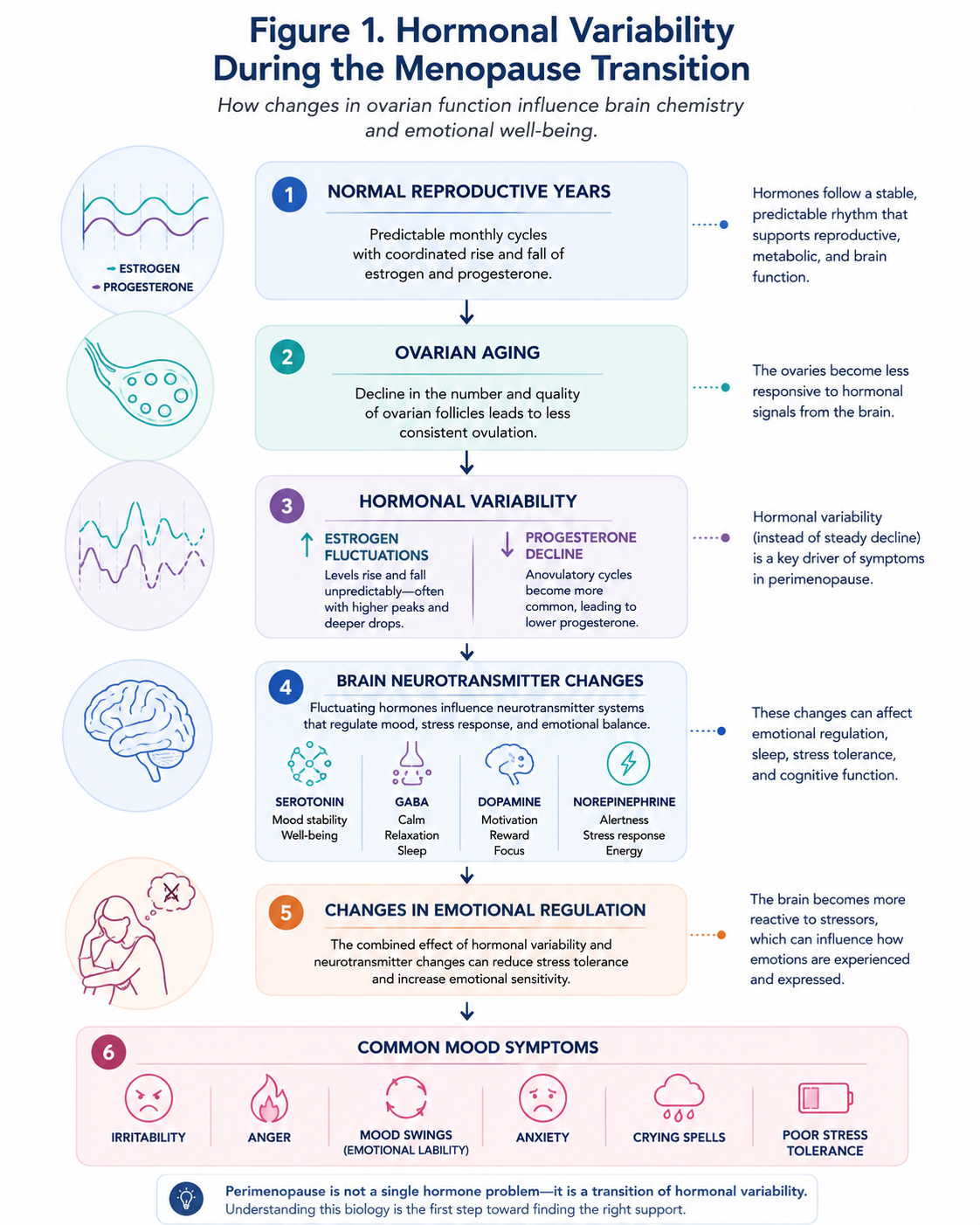
Perimenopause is often discussed in terms of irregular menstrual cycles, hot flashes, and night sweats.
However, the menopause transition is not simply a reproductive event.
It is also a neuroendocrine transition.
Throughout perimenopause, estrogen and progesterone production becomes increasingly unpredictable.
Rather than declining in a steady, gradual fashion, these hormones fluctuate considerably from one cycle to the next—and sometimes even within the same cycle.
These hormonal fluctuations influence far more than the ovaries.
They affect the brain.
Estrogen and progesterone interact with multiple neurotransmitter systems involved in emotional regulation, including serotonin, dopamine, gamma-aminobutyric acid (GABA), and norepinephrine. They also influence stress responsiveness, sleep regulation, cognition, and overall brain function.
As these hormones fluctuate, some women experience increased emotional sensitivity, irritability, anxiety, mood swings, or episodes of intense anger that seem unlike their usual personality.
Importantly, these experiences do not mean that a woman is "losing control," becoming a different person, or failing to cope.
Rather, they often reflect the complex interaction between hormonal changes, brain physiology, sleep quality, chronic stress, metabolic health, and the many demands that frequently accompany midlife.
Understanding this distinction matters.
Recognizing that these symptoms have a biologic basis can reduce self-blame, encourage appropriate evaluation, and help women seek evidence-based strategies that support both their emotional well-being and their long-term health.
Although anger can be a common experience during perimenopause, it is important to recognize that severe or persistent mood symptoms should never be dismissed. Conditions such as premenstrual dysphoric disorder (PMDD), major depressive disorder, generalized anxiety disorder, thyroid disease, iron deficiency, and other medical or psychiatric conditions may produce similar symptoms and deserve appropriate clinical evaluation.
The good news is that women do not have to simply "push through" these changes.
A growing body of research has improved our understanding of how hormonal fluctuations influence the brain during the menopause transition, and effective lifestyle strategies and medical treatments are available for many women.
What This Article Will Cover
In this evidence-based guide, we'll explore:
- Why anger and irritability often become more common during perimenopause.
- How estrogen and progesterone influence the brain and emotional regulation.
- Why mood symptoms frequently worsen before menstruation.
- The relationship between sleep, chronic stress, inflammation, metabolic health, and mood.
- How to distinguish normal hormonal changes from conditions such as PMDD, depression, and anxiety disorders.
- Evidence-based lifestyle and medical approaches that may help support emotional well-being during the menopause transition.
Understanding the biology behind these emotional changes is not about making excuses for them.
It is about replacing confusion with knowledge.
Because when women understand why these changes occur, they are better equipped to seek appropriate care, make informed decisions, and navigate the menopause transition with greater confidence and self-compassion.
Is Anger a Symptom of Perimenopause?
The short answer is yes.
Although hot flashes and irregular menstrual cycles are often considered the hallmark symptoms of perimenopause, emotional and psychological symptoms are also among the most common—and, for many women, among the most distressing.
In fact, many women seek medical care not because of hot flashes, but because they no longer feel like themselves emotionally.
They may notice that they have become unusually irritable.
Their patience seems shorter than it once was.
Minor inconveniences suddenly feel overwhelming.
They become frustrated more easily.
They may snap at loved ones, coworkers, or friends over situations they previously would have handled calmly.
Some women describe episodes of intense anger that seem to appear "out of nowhere," while others experience heightened emotional sensitivity, frequent crying, or persistent anxiety.
These experiences are not uncommon.
Large observational studies have consistently demonstrated that mood-related symptoms become increasingly prevalent during the menopause transition. Women in perimenopause report significantly higher rates of irritability, mood swings, anxiety, and depressive symptoms compared with women who remain in their reproductive years. While not every woman experiences these changes, emotional symptoms are a well-recognized component of the menopause transition.
Common emotional symptoms reported during perimenopause include:
- Irritability
- Impatience
- Frustration
- Anger or increased emotional reactivity
- Mood swings (also called emotional lability)
- Anxiety or excessive worry
- Tearfulness or crying spells
- Feeling emotionally overwhelmed
- Reduced stress tolerance
- Feeling unlike your usual self
Importantly, these symptoms often fluctuate.
Some women feel emotionally well for much of the month but notice a dramatic shift during the days leading up to menstruation.
Others experience more persistent mood changes as menstrual cycles become increasingly irregular.
The pattern varies from woman to woman because hormonal fluctuations during perimenopause are highly individualized.
Mood Symptoms Are Recognized in Major Menopause Guidelines
Emotional symptoms are not simply anecdotal experiences shared on social media.
They are recognized by major professional organizations that develop evidence-based guidance for menopause care.
Organizations such as The Menopause Society (formerly the North American Menopause Society), the International Menopause Society (IMS), the American College of Obstetricians and Gynecologists (ACOG), and the National Institute for Health and Care Excellence (NICE) all acknowledge that changes in mood, anxiety, irritability, and emotional well-being may occur during the menopause transition.
The landmark Study of Women's Health Across the Nation (SWAN) has also provided valuable insight into how emotional symptoms evolve during midlife. This long-term study has shown that the menopause transition represents a period of increased vulnerability to mood symptoms for some women, particularly those with a prior history of depression, significant life stressors, sleep disturbances, or vasomotor symptoms such as hot flashes and night sweats.
These findings have helped shift our understanding of perimenopause.
Rather than viewing it solely as a reproductive transition, researchers increasingly recognize it as a complex neuroendocrine transition that affects multiple organ systems—including the brain.
Why Do These Emotional Changes Occur?
One of the biggest misconceptions about anger during perimenopause is that it reflects a personality change.
Many women worry that they are becoming less patient, less resilient, or somehow "losing control."
In reality, these emotional changes are often rooted in biology.
The brain is highly responsive to reproductive hormones.
Estrogen and progesterone influence the activity of several neurotransmitters—including serotonin, dopamine, gamma-aminobutyric acid (GABA), and norepinephrine—that help regulate mood, emotional resilience, stress responses, sleep, motivation, and cognition.
During perimenopause, hormone production becomes increasingly unpredictable.
Rather than declining smoothly, estrogen levels may fluctuate dramatically from week to week or even day to day. Progesterone production also becomes less consistent as ovulation becomes increasingly irregular.
These hormonal fluctuations can temporarily alter how the brain processes emotions and responds to stress.
For some women, this means feeling emotionally sensitive.
For others, it manifests as increased irritability or episodes of anger.
The emotional response is real, but it is not a reflection of poor character or inadequate coping skills.
It Is Not "Just Hormones"
At the same time, hormones are only one piece of the picture.
Midlife is often accompanied by increasing responsibilities and stressors.
Many women are simultaneously balancing demanding careers, raising children or teenagers, caring for aging parents, managing chronic health conditions, navigating relationship changes, and coping with financial pressures.
Sleep disturbances become more common.
Metabolic changes begin to emerge.
Life stress accumulates.
These physiologic and psychosocial factors interact with hormonal fluctuations, creating what researchers sometimes describe as a "perfect storm" for emotional symptoms.
This helps explain why women who have successfully managed stress throughout much of their lives may suddenly find themselves feeling emotionally overwhelmed during perimenopause.
An Important Message for Women
Perhaps the most important message is this:
Experiencing increased anger, irritability, or emotional sensitivity during perimenopause does not mean you are weak.
It does not mean you are failing.
It does not mean you are "going crazy."
These symptoms are common, biologically plausible, and recognized within the medical literature.
They deserve understanding rather than judgment.
Recognizing that there is a physiologic basis for these changes does not minimize their impact.
Instead, it provides an opportunity to better understand what is happening, seek appropriate evaluation when needed, and explore evidence-based strategies that can help support emotional well-being throughout the menopause transition.
In the next section, we'll explore why these emotional changes occur by examining how estrogen and progesterone communicate with the brain—and why fluctuating hormones can have such a profound effect on mood.
Understanding the Menopause Transition
To understand why anger, irritability, and emotional reactivity can become more common during perimenopause, it is helpful to first understand what is happening inside the ovaries.
Many women assume menopause begins when periods stop.
In reality, the hormonal transition begins years earlier.
This transitional stage is known as perimenopause.
Perimenopause literally means "around menopause."
It represents the gradual transition from the reproductive years to menopause and typically begins during the late 30s or 40s, although the timing varies considerably between women.
For many women, perimenopause lasts four to eight years, though some experience a shorter or longer transition.
During this time, the ovaries are still functioning—but they no longer function with the consistency they did during earlier reproductive life.
Rather than producing hormones in a predictable monthly pattern, hormone production becomes increasingly irregular.
This hormonal variability lies at the heart of many of the physical and emotional symptoms women experience during perimenopause.
The Ovaries Become Less Predictable
Throughout the reproductive years, communication between the brain and the ovaries follows a remarkably coordinated pattern.
The hypothalamus and pituitary gland release hormones that stimulate the ovaries to mature follicles, trigger ovulation, and produce estrogen and progesterone in a relatively predictable cycle.
This tightly regulated system allows hormone levels to rise and fall in an organized rhythm each month.
As women enter perimenopause, however, the number and quality of ovarian follicles gradually decline.
The ovaries become less responsive to hormonal signals from the brain.
Ovulation becomes less consistent.
Some menstrual cycles still involve ovulation.
Others do not.
As a result, hormone production becomes increasingly erratic.
Instead of following the smooth, predictable hormonal patterns seen during the reproductive years, estrogen and progesterone begin fluctuating unpredictably from cycle to cycle—and sometimes even within the same cycle.
These fluctuations are one of the defining biologic features of perimenopause.
Estrogen Does Not Simply Decline—It Fluctuates
One of the biggest misconceptions about perimenopause is that estrogen simply decreases in a straight line.
That is not what typically happens.
Early and mid-perimenopause are often characterized by dramatic fluctuations in estrogen, rather than consistently low estrogen levels.
In fact, estrogen levels may occasionally become higher than those seen during the reproductive years, only to fall rapidly days later.
Researchers have demonstrated that estrogen variability—not simply estrogen deficiency—is an important contributor to many perimenopausal symptoms.
This means a woman may experience significant symptoms even when laboratory estrogen levels appear "normal."
The issue is often the instability of hormone levels rather than a single hormone value measured on one particular day.
These fluctuations can affect multiple organ systems, including:
- The brain
- Blood vessels
- Skin
- Bone
- Muscle
- Sleep regulation
- Body temperature regulation
- Cardiovascular function
The brain is particularly sensitive to these hormonal changes.
We'll explore this relationship in greater detail in the next section.
Progesterone Gradually Declines
Progesterone follows a different pattern.
Unlike estrogen, progesterone production depends almost entirely on ovulation.
After ovulation, the corpus luteum produces progesterone during the second half of the menstrual cycle.
As ovulation becomes less frequent during perimenopause, progesterone production begins to decline.
Many cycles become anovulatory, meaning no egg is released.
Without ovulation, very little progesterone is produced.
This decline in progesterone often begins earlier than the eventual decline in estrogen.
Progesterone has important effects beyond reproduction.
It influences sleep quality, interacts with the brain's gamma-aminobutyric acid (GABA) system, and contributes to feelings of calmness and relaxation in many women.
As progesterone production becomes inconsistent, some women notice:
- Increased irritability
- Poorer sleep
- Heightened anxiety
- Greater emotional sensitivity
- Feeling less able to cope with everyday stress
Although progesterone is only one piece of a much larger picture, its declining production contributes to the changing hormonal environment of perimenopause.
Menstrual Cycles Become Increasingly Irregular
Because hormone production becomes less predictable, menstrual cycles also begin to change.
For many women, this is the first noticeable sign of perimenopause.
Periods may become:
- Earlier than expected
- Delayed
- Longer
- Shorter
- Heavier
- Lighter
- More unpredictable from month to month
Some women experience skipped periods.
Others have cycles that seem completely normal for months before suddenly becoming irregular again.
This variability reflects the changing function of the ovaries rather than a steady progression toward menopause.
Eventually, as ovarian function continues to decline, estrogen production decreases more consistently, ovulation ceases permanently, and menstruation stops.
Menopause is officially diagnosed after 12 consecutive months without a menstrual period, assuming no other medical explanation.
Why Hormonal Variability Matters More Than Hormone Levels
One of the most important concepts in understanding perimenopause is that the brain responds not only to hormone levels but also to how rapidly those levels change.
Think of the hormonal environment during the reproductive years as calm, predictable waves.
During perimenopause, those waves become increasingly turbulent.
The brain must continually adapt to rapidly changing hormonal signals.
For some women, this adaptation occurs with relatively few symptoms.
For others, these fluctuations contribute to significant changes in mood, sleep, cognition, temperature regulation, and emotional resilience.
This is why two women of the same age—or even the same woman during different months—may have very different experiences.
Perimenopause is not a single hormonal state.
It is a dynamic transition characterized by ongoing hormonal variability.
Understanding this biology helps explain why emotional symptoms can appear long before menstruation stops and why many women feel that their emotional experiences become increasingly unpredictable during midlife.
In the next section, we'll examine how fluctuating estrogen and progesterone influence key neurotransmitters in the brain—and why these changes can contribute to irritability, anger, anxiety, and mood swings during perimenopause.
Clinical Pearl
Perhaps the most important concept to remember is this:
Perimenopause is characterized by hormonal variability—not simply low hormone levels.
For many women, it is these unpredictable hormonal fluctuations, rather than menopause itself, that drive many of the emotional symptoms experienced during the transition.
Why Does Anger Often Happen Before My Period?
For many women, one of the most confusing aspects of perimenopause is not simply that they feel more emotional—it is when those emotions occur.
Many describe feeling relatively well for most of the month.
Then, seemingly without warning, everything changes.
Patience becomes scarce.
Minor inconveniences suddenly feel unbearable.
They become unusually irritable.
Small disagreements escalate more quickly.
Some experience intense anger over situations they would normally handle calmly.
Others find themselves crying unexpectedly or feeling overwhelmed by emotions they cannot fully explain.
Perhaps the most common description is this:
"I'm fine for most of the month...then about a week before my period I become a completely different person."
This experience is remarkably common.
It is also biologically understandable.
For many women, these symptoms occur during the late luteal phase of the menstrual cycle—the days between ovulation and the start of menstruation.
During perimenopause, this phase becomes increasingly unstable because hormone levels fluctuate more dramatically than they did during earlier reproductive life.
Understanding what happens during the late luteal phase helps explain why anger often appears just before menstruation.
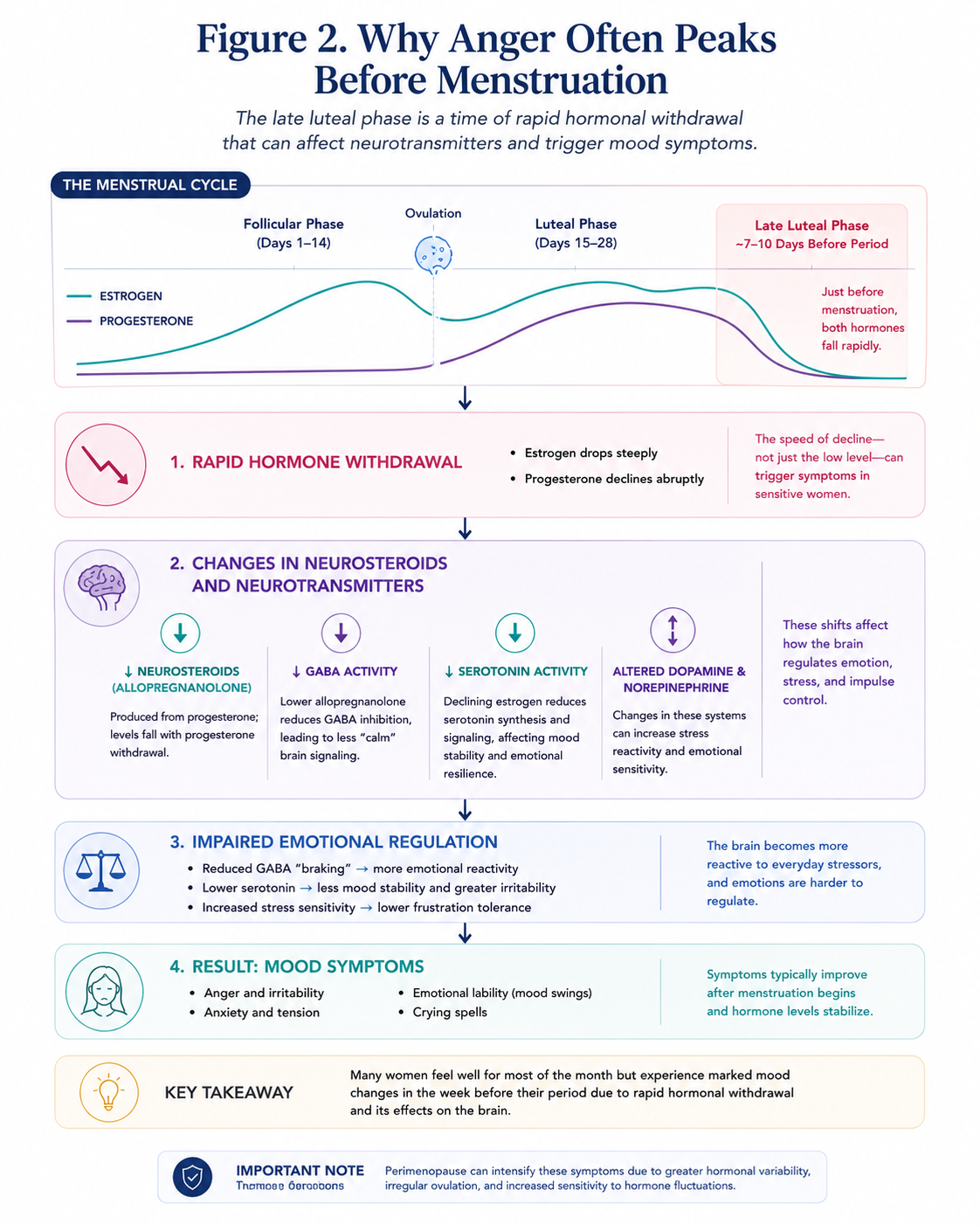
The Late Luteal Phase: A Time of Rapid Hormonal Change
The menstrual cycle consists of several phases, each characterized by distinct hormonal patterns.
Following ovulation, the body enters the luteal phase.
During this phase:
- Progesterone reaches its highest levels.
- Estrogen rises again to a smaller secondary peak.
- The body prepares for a possible pregnancy.
If pregnancy does not occur, hormone production begins to decline.
During the late luteal phase, both estrogen and progesterone fall rapidly.
For women in their reproductive years, this hormonal withdrawal occurs in a relatively predictable pattern.
During perimenopause, however, hormone production is far less consistent.
Ovulation may occur one month but not the next.
Progesterone production may be reduced.
Estrogen may fluctuate dramatically before falling.
As a result, the brain is exposed to greater hormonal instability.
For women who are particularly sensitive to these hormonal changes, this period can trigger significant emotional symptoms.
It Is the Change That Matters
An important concept in menopause medicine is that many women are not reacting to low hormone levels alone.
Instead, they are reacting to rapid hormonal change.
Research suggests that some women have brains that are especially sensitive to fluctuations in reproductive hormones.
This helps explain why two women with similar hormone levels can have very different experiences.
It also explains why symptoms often appear suddenly.
The brain continuously adapts to changing estrogen and progesterone levels.
When those changes become more abrupt during perimenopause, emotional regulation may become temporarily more difficult.
Rather than a gradual shift in mood, women may experience rapid changes over just a few days.
Estrogen Withdrawal and the Brain
Estrogen has important effects on multiple neurotransmitter systems involved in emotional regulation.
These include:
- Serotonin
- Dopamine
- Norepinephrine
Estrogen helps support serotonin production and activity.
Serotonin plays a major role in:
- Mood stability
- Emotional resilience
- Impulse control
- Anxiety regulation
- Sleep
As estrogen declines during the late luteal phase, serotonin signaling may become less efficient in susceptible women.
This may contribute to:
- Increased irritability
- Lower frustration tolerance
- Anxiety
- Sadness
- Emotional sensitivity
Researchers believe this is one reason emotional symptoms often become more noticeable just before menstruation.
## Progesterone Withdrawal and Neurosteroids
Progesterone influences the brain differently.
One of its most important effects occurs through its conversion into allopregnanolone, a naturally occurring neurosteroid.
Allopregnanolone enhances the activity of gamma-aminobutyric acid (GABA), the brain's primary inhibitory neurotransmitter.
GABA helps regulate:
- Calmness
- Relaxation
- Stress responses
- Emotional stability
- Sleep
You can think of GABA as one of the brain's natural "braking systems."
It helps prevent the nervous system from becoming excessively activated.
When progesterone declines before menstruation, allopregnanolone levels also fall.
For many women, this reduction decreases GABA activity.
The result may be:
- Feeling emotionally "on edge"
- Increased irritability
- Greater emotional reactivity
- Heightened anxiety
- Poor stress tolerance
- Difficulty sleeping
Some women appear to be especially sensitive to changes in allopregnanolone rather than to the absolute amount present.
This sensitivity is an active area of research and is believed to play an important role in disorders such as premenstrual dysphoric disorder (PMDD).
Multiple Neurotransmitters Are Affected
Although serotonin receives much of the attention, emotional regulation depends on the coordinated activity of many neurotransmitters.
During the late luteal phase, fluctuating reproductive hormones may influence several important brain systems simultaneously.
These include:
Serotonin
- Mood regulation
- Emotional stability
- Anxiety
- Sleep
GABA
- Calmness
- Relaxation
- Stress tolerance
- Emotional control
Dopamine
- Motivation
- Reward
- Focus
- Energy
Norepinephrine
- Alertness
- Stress response
- Attention
- Emotional arousal
Rather than affecting a single pathway, hormonal fluctuations influence an interconnected network of brain systems.
This helps explain why symptoms rarely occur in isolation.
A woman experiencing increased anger before her period may also notice:
- Poor sleep
- Fatigue
- Anxiety
- Difficulty concentrating
- Increased sensitivity to stress
- Reduced patience
- Feeling emotionally overwhelmed
Why Perimenopause Can Make Premenstrual Symptoms Worse
Many women report that they had only mild premenstrual symptoms in their twenties or thirties.
Then, during their forties, those symptoms suddenly become much more intense.
This is a well-recognized pattern.
As hormonal fluctuations become more pronounced during perimenopause, women who were previously minimally affected may become increasingly sensitive to the rapid hormonal shifts occurring before menstruation.
In addition, many women are simultaneously experiencing:
- Sleep disruption
- Chronic stress
- Caregiving responsibilities
- Demanding careers
- Parenting adolescents
- Aging parents
- Metabolic changes
Each of these factors can reduce the brain's ability to tolerate physiologic stress.
Hormonal fluctuations occur against this broader backdrop, making emotional symptoms feel even more intense.
Anger Is Often a Symptom of Neurobiology, Not Character
Perhaps the most reassuring message for many women is this:
Feeling unusually angry before your period does not mean you have become an angry person.
It does not mean you lack self-control.
It does not mean you are failing emotionally.
For many women, these experiences reflect the interaction between fluctuating reproductive hormones, neurotransmitter systems, sleep, stress physiology, and the unique sensitivity of the brain during the menopause transition.
Recognizing this biology can be profoundly validating.
Understanding why these changes occur is the first step toward identifying effective strategies to reduce their impact.
Clinical Pearl
Many women are not reacting to low hormone levels—they are reacting to rapid hormonal withdrawal.
This distinction helps explain why symptoms often appear predictably during the week before menstruation and why they can become more pronounced during perimenopause, when hormonal fluctuations are greater and less predictable.
The Brain During Perimenopause
Perhaps one of the most important concepts women should understand is this:
Perimenopause is not simply a reproductive transition—it is also a neurologic transition.
Although menopause is often discussed in terms of the ovaries, the brain is one of the primary organs affected by changing reproductive hormones.
This is because estrogen does far more than regulate the menstrual cycle.
Throughout a woman's reproductive years, estrogen acts as a powerful neuromodulator, influencing how brain cells communicate, adapt, and respond to stress.
Neuroscientists sometimes refer to estrogen as one of the brain's "master regulators" because it affects multiple neurotransmitter systems simultaneously.
As estrogen fluctuates during perimenopause, these widespread effects on the brain begin to change.
This helps explain why many women notice several symptoms occurring together, including:
- Irritability
- Anger
- Anxiety
- Brain fog
- Poor concentration
- Sleep disturbance
- Fatigue
- Mood swings
- Reduced stress tolerance
Rather than representing unrelated problems, these symptoms often reflect changes occurring within the same interconnected neural networks.
Estrogen Is Active Throughout the Brain
Estrogen receptors are found throughout numerous brain regions involved in emotional regulation and cognitive function.
These include areas responsible for:
- Emotional processing
- Executive function
- Learning and memory
- Sleep regulation
- Stress responses
- Motivation
- Decision-making
Among the most important regions are:
- Prefrontal cortex, which supports judgment, impulse control, planning, and emotional regulation.
- Amygdala, which detects emotional threats and generates fear and anger responses.
- Hippocampus, which plays a central role in memory formation and learning.
- Hypothalamus, which regulates sleep, temperature, circadian rhythms, and many hormonal functions.
Because estrogen influences all of these brain regions, fluctuations can affect emotional, cognitive, and physical symptoms simultaneously.
Estrogen and Serotonin
Serotonin is perhaps the neurotransmitter most closely associated with mood.
It helps regulate:
- Emotional stability
- Anxiety
- Impulse control
- Sleep
- Appetite
- Overall sense of well-being
Estrogen supports serotonin function through several mechanisms.
Research suggests estrogen can:
- Increase serotonin synthesis.
- Influence serotonin receptor activity.
- Reduce serotonin breakdown.
- Enhance serotonin signaling between neurons.
When estrogen fluctuates or declines during perimenopause, serotonin signaling may become less efficient.
For some women, this contributes to:
- Irritability
- Increased emotional sensitivity
- Anxiety
- Depressed mood
- Reduced frustration tolerance
These changes are one reason selective serotonin reuptake inhibitors (SSRIs) may improve certain menopausal mood symptoms and are considered an evidence-based treatment for women with significant depressive or vasomotor symptoms.
Estrogen and Dopamine
Dopamine is involved in:
- Motivation
- Reward
- Focus
- Attention
- Energy
- Goal-directed behavior
Many women describe feeling less motivated during perimenopause.
Tasks that once seemed manageable may suddenly feel mentally exhausting.
Some notice difficulty initiating projects.
Others lose interest in activities they previously enjoyed.
Although multiple factors contribute—including sleep disruption and stress—changing estrogen levels also influence dopamine pathways within the brain.
Researchers believe estrogen helps modulate dopamine production and receptor activity, particularly in regions involved in executive functioning and motivation.
This may help explain why some women simultaneously experience:
- Brain fog
- Reduced motivation
- Difficulty concentrating
- Emotional fatigue
Estrogen and Norepinephrine
Norepinephrine plays an important role in:
- Alertness
- Attention
- Stress responses
- Cognitive performance
- Emotional arousal
It is closely linked with the body's "fight-or-flight" response.
Fluctuating estrogen levels may alter norepinephrine activity within the brain.
As a result, some women become more reactive to everyday stressors.
Situations that previously felt manageable may suddenly feel overwhelming.
Women often describe feeling:
- Easily startled
- More emotionally reactive
- Less patient
- More easily overwhelmed
- Unable to "bounce back" after stressful events
This increased stress sensitivity often occurs alongside changes in serotonin and GABA signaling, amplifying emotional symptoms.
Estrogen, GABA, and Emotional Calm
While progesterone primarily influences GABA through its neurosteroid metabolite allopregnanolone, estrogen also interacts with GABAergic signaling.
GABA is the brain's principal inhibitory neurotransmitter.
Its primary role is to prevent excessive neuronal activity.
Healthy GABA function supports:
- Relaxation
- Emotional regulation
- Calmness
- Sleep
- Reduced anxiety
During perimenopause, fluctuating estrogen and declining progesterone can alter GABA signaling.
The result may be a nervous system that feels more easily activated.
Women often describe this as:
- Feeling "on edge"
- Feeling emotionally overstimulated
- Increased anxiety
- Difficulty relaxing
- Poor stress tolerance
These symptoms often worsen during periods of sleep deprivation or chronic stress.
Estrogen and Glutamate
If GABA acts as the brain's braking system, glutamate functions as its primary excitatory neurotransmitter.
Glutamate is essential for:
- Learning
- Memory
- Synaptic plasticity
- Information processing
Balanced communication between glutamate and GABA allows the brain to function efficiently.
Estrogen helps regulate this balance.
When estrogen fluctuates significantly, communication between excitatory and inhibitory pathways may become less stable.
Researchers believe this altered balance may contribute to:
- Cognitive fatigue
- Difficulty concentrating
- Heightened emotional responses
- Sleep disruption
- Increased anxiety
Although glutamate receives less public attention than serotonin, it is increasingly recognized as an important contributor to cognitive and emotional symptoms during the menopause transition.
Estrogen Supports Communication Between Brain Cells
Perhaps the most fascinating role of estrogen extends beyond individual neurotransmitters.
Estrogen helps brain cells communicate efficiently.
It influences:
- Synaptic plasticity
- Formation of new neuronal connections
- Neural signaling efficiency
- Neuroprotection
- Energy metabolism within brain cells
- Cerebral blood flow
In other words, estrogen helps optimize the way neural networks function.
As estrogen becomes increasingly variable during perimenopause, these communication networks must continually adapt.
This does not mean the brain is damaged.
Rather, it reflects a period of neurologic remodeling.
For some women, this adaptation occurs with relatively few symptoms.
For others, it manifests as noticeable changes in mood, memory, attention, sleep, and emotional resilience.
Why So Many Symptoms Occur Together
One of the most reassuring insights for women is understanding that mood symptoms rarely occur in isolation.
The same hormonal fluctuations influencing serotonin may also affect dopamine, norepinephrine, GABA, glutamate, sleep regulation, and stress physiology.
This explains why a woman may simultaneously experience:
- Anger
- Anxiety
- Brain fog
- Poor concentration
- Insomnia
- Fatigue
- Emotional sensitivity
- Reduced resilience to stress
These symptoms are interconnected because they arise from shared neurobiological pathways rather than separate medical problems.
Understanding this broader neurologic perspective helps explain why perimenopause can feel so different from anything a woman has previously experienced.
It is not simply a reproductive transition.
It is a whole-brain transition.
Clinical Pearl
Perimenopause is not simply about changing hormone levels—it is about how changing hormones influence the brain.
Because estrogen affects multiple neurotransmitter systems simultaneously, mood, cognition, sleep, and anxiety often occur together rather than as isolated symptoms.
Why Small Things Suddenly Feel So Big
Perhaps one of the most frustrating experiences women describe during perimenopause is not simply feeling more emotional—it is feeling as though their emotional reactions no longer match the situation.
A forgotten grocery item.
An email.
A crying child.
A spouse asking a simple question.
Traffic.
Noise.
Someone chewing too loudly.
The dishwasher breaking.
An unexpected meeting.
A small inconvenience that once would have been brushed aside suddenly feels overwhelming.
Many women say:
"I know I'm overreacting, but I can't seem to stop it."
Others describe feeling emotionally exhausted before the day has even begun.
These experiences can be deeply unsettling.
Some begin questioning their personality.
Others wonder whether they are "losing patience" or becoming an angry person.
Fortunately, neuroscience offers a different explanation.
For many women, these reactions reflect changes in emotional regulation, stress tolerance, and the brain's ability to manage cognitive demands during the menopause transition.
Emotional Regulation: The Brain's Internal Control System
Emotional regulation refers to the brain's ability to recognize emotions, interpret them appropriately, and respond in a balanced way.
Healthy emotional regulation allows us to:
- Pause before reacting.
- Put situations into perspective.
- Recover after stressful events.
- Tolerate frustration.
- Shift attention away from negative thoughts.
- Maintain perspective during conflict.
This process depends heavily on communication between the prefrontal cortex and the amygdala.
The prefrontal cortex functions as the brain's executive control center.
It helps us think logically, weigh consequences, solve problems, and regulate emotional responses.
The amygdala, in contrast, rapidly detects emotionally significant or potentially threatening situations.
Under normal circumstances, these regions work together.
The amygdala generates an emotional response.
The prefrontal cortex evaluates that response and determines whether it is proportionate.
When hormonal fluctuations, sleep disruption, chronic stress, and neurotransmitter changes occur simultaneously, this balance can become less efficient.
The emotional response becomes louder.
The brain's regulatory "brakes" become less effective.
As a result, emotions may feel more intense and more difficult to control.
Stress Tolerance Changes During Perimenopause
Stress tolerance refers to the amount of physical or emotional stress the brain can manage before becoming overwhelmed.
Every individual has a finite capacity to process stress.
During the reproductive years, many women can absorb multiple daily stressors without feeling emotionally overloaded.
During perimenopause, however, that reserve may become smaller.
Hormonal variability influences neurotransmitters involved in stress regulation.
Sleep quality often declines.
Night sweats and insomnia become more common.
Caregiving responsibilities may increase.
Professional responsibilities often peak during the same stage of life.
Many women are simultaneously raising children, supporting aging parents, advancing their careers, and managing their own health concerns.
Each of these demands consumes mental and emotional resources.
The result is a brain that reaches its stress threshold more quickly.
What previously felt manageable may suddenly feel exhausting.
Understanding Cognitive Load
One concept that helps explain this experience is cognitive load.
Cognitive load refers to the total amount of mental effort the brain is using at any given time.
The brain is constantly processing information.
It is making decisions.
Planning.
Remembering appointments.
Managing work.
Monitoring children.
Regulating emotions.
Responding to emails.
Solving problems.
Filtering distractions.
Most of this occurs without conscious awareness.
As cognitive load increases, fewer mental resources remain available for emotional regulation.
Imagine carrying a backpack.
Each responsibility adds another item.
Work deadlines.
Family responsibilities.
Financial concerns.
Sleep deprivation.
Hormonal fluctuations.
By the end of the day, the backpack has become significantly heavier.
Adding one more small stressor may not seem important in isolation—but when the backpack is already full, even a light object can feel impossible to carry.
The same principle applies to the brain.
Often, the problem is not the final stressor itself.
It is the cumulative cognitive load that came before it.
Executive Function Requires Energy
Executive function refers to the brain's higher-order cognitive abilities.
These include:
- Planning
- Decision-making
- Organization
- Attention
- Working memory
- Flexible thinking
- Impulse control
- Emotional regulation
These abilities rely heavily on the prefrontal cortex.
Executive function is remarkably sensitive to physiologic stress.
Sleep deprivation.
Hormonal fluctuations.
Chronic stress.
Inflammation.
Fatigue.
Poor nutrition.
Each can reduce executive functioning.
When executive function is compromised, everyday tasks require greater mental effort.
Decision-making feels harder.
Patience becomes more limited.
Concentration declines.
The brain becomes less efficient at shifting attention away from emotionally charged situations.
As a result, relatively small frustrations may trigger disproportionately large emotional responses.
Sleep Deprivation Magnifies Emotional Reactivity
Sleep deserves special attention because it has profound effects on emotional regulation.
Many women entering perimenopause experience:
- Difficulty falling asleep
- Frequent nighttime awakenings
- Early morning awakening
- Night sweats
- Less restorative sleep
Even modest reductions in sleep quality can alter how the brain processes emotions.
Functional neuroimaging studies have demonstrated that sleep deprivation increases amygdala reactivity while reducing regulatory input from the prefrontal cortex.
In practical terms, the emotional "accelerator" becomes stronger while the emotional "brakes" become weaker.
This helps explain why women often notice that everything feels more difficult after a poor night's sleep.
The issue is not simply fatigue.
It is altered emotional processing.
Chronic Stress Changes the Brain
Stress itself is not harmful.
The problem is persistent, unrelenting stress without adequate recovery.
Repeated activation of the body's stress response affects multiple physiologic systems, including:
- Cortisol regulation
- Inflammation
- Autonomic nervous system activity
- Sleep architecture
- Brain connectivity
Over time, chronic stress may reduce resilience.
The brain becomes increasingly vigilant.
Minor stressors are interpreted as larger threats.
Emotional recovery takes longer.
Hormonal variability during perimenopause occurs against this backdrop.
Rather than acting alone, fluctuating estrogen and progesterone interact with existing physiologic stress, amplifying emotional symptoms in susceptible women.
Hormonal Variability Lowers the Threshold
Perhaps the most important concept is that perimenopause does not necessarily create emotional reactions from nothing.
Instead, it often lowers the threshold at which emotional responses occur.
Imagine a smoke detector.
When functioning appropriately, it activates when there is a true fire.
If the detector becomes overly sensitive, however, it may alarm when someone simply burns toast.
The smoke detector is not broken.
Its threshold has changed.
Similarly, during perimenopause, the brain may become more sensitive to everyday stressors.
The stressor itself has not changed.
The brain's response to that stressor has.
This is why:
- A delayed email suddenly feels deeply upsetting.
- Household noise feels intolerable.
- A simple disagreement escalates into an argument.
- Everyday frustrations seem disproportionately overwhelming.
Understanding this distinction can be incredibly validating.
The goal is not to dismiss these emotions.
The emotions are real.
What changes is the brain's capacity to regulate them under the combined influence of hormonal variability, sleep disruption, cognitive load, and chronic stress.
The Bigger Picture
For many women, the overwhelming feeling is not caused by one isolated event.
It is the result of multiple biologic and environmental factors converging at the same time.
Hormonal variability influences neurotransmitters.
Poor sleep reduces emotional regulation.
Chronic stress increases physiologic arousal.
High cognitive load consumes mental resources.
Executive function becomes less efficient.
Together, these changes lower emotional resilience.
Understanding this broader physiologic framework allows women to replace self-blame with self-understanding.
It shifts the question from:
"Why am I overreacting?"
to
"What is my brain managing right now?"
That shift in perspective is often one of the most empowering lessons of the menopause transition.
Clinical Pearl
Perimenopause does not necessarily make women more emotional—it often makes the brain work harder to regulate emotions while simultaneously increasing the number of physiologic and cognitive demands placed upon it.
When hormonal variability, poor sleep, chronic stress, and high cognitive load occur together, even small frustrations can feel disproportionately overwhelming—not because of personal weakness, but because the brain is operating with a reduced reserve.
Why Sleep Makes Everything Worse
If there is one factor that consistently amplifies mood symptoms during perimenopause, it is poor sleep.
Many women notice a predictable pattern.
After a good night's sleep, they feel more patient.
More resilient.
Better able to cope with everyday challenges.
After a poor night's sleep, however, everything feels harder.
Small frustrations become major frustrations.
Patience disappears.
Concentration declines.
Emotions feel closer to the surface.
Many women conclude that the problem is simply fatigue.
In reality, the effects of sleep deprivation extend far beyond feeling tired.
Sleep is one of the brain's most important mechanisms for restoring emotional regulation, cognitive performance, memory consolidation, and stress resilience.
When sleep becomes disrupted during perimenopause, the brain loses one of its most powerful tools for maintaining emotional balance.
Sleep Disturbance Is Extremely Common During Perimenopause
Sleep problems are among the most frequently reported symptoms during the menopause transition.
Research suggests that 40–60% of women experience clinically significant sleep disturbances during perimenopause and menopause, making sleep one of the most common concerns reported during midlife.
Women may experience:
- Difficulty falling asleep
- Frequent nighttime awakenings
- Early morning awakening
- Restless sleep
- Night sweats
- Reduced sleep quality despite adequate sleep duration
- Feeling unrefreshed upon waking
Importantly, sleep disturbances often begin before menopause itself, during the years of hormonal fluctuation known as perimenopause.
For many women, sleep disruption becomes one of the earliest signs that hormonal changes are occurring.
Why Do So Many Women Wake at 3 AM?
One of the most common questions women ask is:
"Why do I keep waking up around 3 AM?"
This experience is remarkably common during perimenopause.
Several physiologic mechanisms may contribute.
Hormonal Variability
Estrogen influences multiple brain regions involved in sleep regulation, including those that regulate circadian rhythms and body temperature.
As estrogen fluctuates, sleep architecture may become less stable.
Women may transition more easily from deeper stages of sleep into lighter sleep, making nighttime awakenings more frequent.
Declining Progesterone
Progesterone has mild sedative and anxiolytic properties.
Its metabolite, allopregnanolone, enhances GABA activity within the brain, promoting relaxation and sleep.
As ovulation becomes less consistent during perimenopause, progesterone production declines.
Lower progesterone may contribute to:
- Difficulty falling asleep
- More fragmented sleep
- Reduced sleep efficiency
Night Sweats and Vasomotor Symptoms
Fluctuating estrogen affects the hypothalamus, the brain's temperature-regulating center.
This narrows the body's thermoneutral zone, making small changes in core body temperature more likely to trigger:
- Night sweats
- Hot flashes
- Sudden awakenings
Even when women do not fully remember waking, repeated sleep interruptions reduce overall sleep quality.
Cortisol and Early Morning Awakening
Cortisol follows a normal circadian rhythm.
Levels gradually rise during the early morning hours, preparing the body to wake.
However, chronic stress, anxiety, and sleep disruption can alter this rhythm.
Some researchers believe that increased nighttime physiologic arousal may contribute to the characteristic early morning awakenings experienced by many women during perimenopause.
Women often report waking around 2–4 AM with:
- A racing mind
- Difficulty returning to sleep
- Heightened anxiety
- Increased awareness of worries or responsibilities
While cortisol is only one piece of a much more complex picture, changes in stress physiology likely interact with hormonal variability to worsen sleep quality.
Sleep Restores Emotional Regulation
Sleep is not simply a period of rest.
It is an active biologic process during which the brain performs essential maintenance.
During healthy sleep, the brain:
- Consolidates memories
- Regulates neurotransmitters
- Restores metabolic balance
- Clears cellular waste products
- Replenishes energy stores
- Processes emotional experiences
Sleep also helps recalibrate the neural circuits responsible for emotional regulation.
This daily "reset" allows us to respond more calmly to challenges the following day.
When sleep is repeatedly interrupted, that reset becomes incomplete.
The brain begins operating with fewer emotional reserves.
What Happens to the Brain After Poor Sleep?
Modern neuroimaging studies have transformed our understanding of sleep deprivation.
Researchers have shown that inadequate sleep alters communication between key brain regions responsible for emotional regulation.
One of the most important findings involves the relationship between the amygdala and the prefrontal cortex.
The amygdala functions as the brain's emotional alarm system.
It rapidly detects potential threats and generates emotional responses.
The prefrontal cortex helps regulate those responses by applying judgment, perspective, and impulse control.
Following sleep deprivation, studies have demonstrated:
- Increased amygdala reactivity
- Reduced functional connectivity between the amygdala and prefrontal cortex
- Impaired emotional regulation
- Increased emotional intensity
- Greater sensitivity to negative experiences
In simple terms, the emotional "accelerator" becomes more active while the emotional "brakes" become less effective.
This helps explain why relatively minor frustrations can feel overwhelming after a poor night's sleep.
Sleep Deprivation Increases Stress Reactivity
Sleep loss also affects the body's stress response.
After insufficient sleep, individuals often demonstrate:
- Higher emotional reactivity
- Reduced frustration tolerance
- Increased anxiety
- Poorer concentration
- Slower cognitive processing
- Reduced resilience during stressful situations
For women already experiencing hormonal variability, these changes can amplify mood symptoms even further.
Hormonal fluctuations and sleep deprivation often reinforce one another in a self-perpetuating cycle.
Poor sleep increases emotional reactivity.
Greater emotional distress makes it harder to sleep.
Repeated nights of fragmented sleep further reduce emotional resilience.
Breaking this cycle is often an important part of improving overall well-being during perimenopause.
Sleep, Mood, and Cognitive Function Are Closely Connected
One reason women often experience multiple symptoms simultaneously is that sleep influences nearly every major brain function.
Poor sleep can contribute to:
- Irritability
- Anger
- Anxiety
- Brain fog
- Difficulty concentrating
- Poor memory
- Reduced motivation
- Fatigue
- Lower stress tolerance
These symptoms frequently overlap because they arise from interconnected neurobiological pathways rather than isolated problems.
This is one reason improving sleep often leads to improvements in mood, cognition, and emotional resilience—even before other symptoms fully resolve.
Sleep Should Be Considered Part of Perimenopause Care
Because sleep affects nearly every aspect of physical and mental health, addressing sleep disturbances should be considered an essential component of comprehensive perimenopause care.
Improving sleep may involve:
- Optimizing sleep hygiene
- Managing vasomotor symptoms
- Treating underlying sleep disorders when present
- Addressing stress and anxiety
- Optimizing physical activity
- Evaluating hormonal and non-hormonal treatment options when appropriate
For many women, improving sleep is one of the highest-yield interventions for improving overall quality of life during the menopause transition.
If you'd like to learn more about why so many women wake during the early morning hours, you may also enjoy our article:
→ Why Am I Waking Up at 3 AM in My 40s? Understanding Sleep During Perimenopause
Clinical Pearl
Sleep does not simply influence how tired you feel—it influences how your brain processes emotions.
During perimenopause, hormonal variability, night sweats, early morning awakening, and chronic stress can disrupt sleep. In turn, poor sleep increases amygdala reactivity, reduces emotional regulation by the prefrontal cortex, and lowers stress tolerance, making everyday frustrations feel much more overwhelming than they otherwise would.
Blood Sugar, Nutrition, and Mood
Although hormonal fluctuations play a central role in the mood changes experienced during perimenopause, they do not act in isolation.
The brain is one of the body's most metabolically active organs. It depends on a continuous supply of oxygen, glucose, amino acids, vitamins, minerals, and essential fatty acids to produce neurotransmitters, generate energy, and regulate emotional responses.
When these physiologic needs are not consistently met, the brain becomes less resilient to the hormonal fluctuations already occurring during the menopause transition.
This helps explain why some women notice that their irritability is significantly worse on days when they skip meals, eat very little protein, experience poor sleep, or are under prolonged stress.
Importantly, nutritional deficiencies and metabolic changes are not the sole cause of mood symptoms during perimenopause. Rather, they may amplify symptoms in women who are already experiencing hormonal variability.
Understanding these contributors allows for a more comprehensive approach to improving emotional well-being.
Blood Sugar Stability and Emotional Regulation
The brain consumes approximately 20% of the body's energy despite accounting for only about 2% of total body weight.
Unlike many other organs, the brain has limited energy reserves and depends on a relatively constant supply of glucose.
Large fluctuations in blood glucose may temporarily impair cognitive function and emotional regulation.
When blood sugar falls rapidly, the body responds by releasing counter-regulatory hormones, including:
- Epinephrine (adrenaline)
- Norepinephrine
- Cortisol
- Glucagon
These hormones help restore blood glucose levels but may also produce symptoms such as:
- Irritability
- Anxiety
- Feeling "on edge"
- Trembling
- Difficulty concentrating
- Increased emotional sensitivity
Many women describe becoming disproportionately angry or emotionally reactive after skipping meals or eating foods that cause rapid spikes and crashes in blood sugar.
While these symptoms are not unique to perimenopause, hormonal fluctuations may reduce the brain's resilience, making blood sugar instability feel even more pronounced during midlife.
Why Skipping Meals Can Make Mood Worse
Many busy women unintentionally go long periods without eating.
Work meetings.
Caring for children.
Running errands.
Back-to-back responsibilities.
By the time they finally eat, they may already feel exhausted, irritable, and emotionally depleted.
Prolonged fasting during the day can contribute to:
- Greater fluctuations in blood glucose
- Increased cortisol secretion
- Increased hunger later in the day
- Poorer food choices
- Reduced concentration
- Lower frustration tolerance
This does not mean that every woman should avoid intermittent fasting. Some women tolerate structured fasting well, while others notice worsening mood, headaches, or irritability.
The key is recognizing that nutritional strategies should be individualized, particularly during the menopause transition.
For women experiencing significant mood symptoms, consistently nourishing the brain with balanced meals may help reduce physiologic stress.
Insulin Resistance During Perimenopause
Perimenopause is also associated with important metabolic changes.
As estrogen levels fluctuate and gradually decline, women often experience:
- Reduced insulin sensitivity
- Increased visceral fat accumulation
- Changes in body composition
- Greater difficulty maintaining stable blood glucose
Insulin resistance does not develop in every woman, but it becomes increasingly common during midlife.
When insulin sensitivity declines, larger fluctuations in blood glucose may occur throughout the day.
These metabolic changes may contribute not only to weight gain but also to fatigue, reduced energy, and diminished cognitive performance.
Because the brain relies heavily on glucose metabolism, maintaining metabolic health may support both physical and emotional well-being.
The Importance of Adequate Protein Intake
Protein provides the amino acids needed to synthesize many of the neurotransmitters involved in mood regulation.
For example:
- Tryptophan is required for serotonin production.
- Tyrosine serves as a precursor for dopamine and norepinephrine.
Although simply eating more protein does not directly increase neurotransmitter levels, consistently consuming adequate dietary protein supports normal neurotransmitter synthesis and overall brain health.
Protein also helps:
- Improve satiety
- Reduce rapid blood sugar fluctuations
- Support muscle maintenance
- Preserve lean body mass during perimenopause
Because skeletal muscle is a major site of glucose disposal, maintaining muscle mass through adequate protein intake and resistance training may also support metabolic health.
---
Iron Deficiency and Mood
Iron deficiency is common among women who continue to menstruate, particularly those with heavy or prolonged periods.
Iron plays an essential role in:
- Oxygen transport
- Cellular energy production
- Dopamine synthesis
- Brain function
Even before anemia develops, iron deficiency may contribute to symptoms such as:
- Fatigue
- Reduced exercise tolerance
- Difficulty concentrating
- Brain fog
- Reduced cognitive performance
Some studies also suggest an association between iron deficiency and mood disturbances, although the relationship is complex and multifactorial.
For women with heavy menstrual bleeding, evaluating iron status may be an important part of a comprehensive assessment.
Vitamin D and Emotional Health
Vitamin D receptors are present throughout multiple regions of the brain.
Researchers continue to investigate the relationship between vitamin D and mood regulation.
Some observational studies have reported associations between low vitamin D levels and depressive symptoms, although randomized clinical trials have produced mixed results.
Current evidence does not support vitamin D supplementation solely as a treatment for mood symptoms in otherwise healthy individuals.
However, correcting true vitamin D deficiency remains important for:
- Bone health
- Muscle function
- Immune health
- Overall health during midlife
Women at increased risk for deficiency may benefit from discussing appropriate testing with their healthcare professional.
Magnesium
Magnesium participates in hundreds of enzymatic reactions throughout the body.
Within the nervous system, magnesium influences:
- NMDA receptor activity
- GABA function
- Neuronal excitability
- Muscle relaxation
Research evaluating magnesium supplementation for anxiety and mood remains limited, and results have been inconsistent.
However, maintaining adequate magnesium intake through diet—and correcting deficiency when present—supports overall physiologic function.
Women with low dietary intake, gastrointestinal disorders, or certain medical conditions may be at increased risk for deficiency.
Omega-3 Fatty Acids
Omega-3 fatty acids, particularly EPA and DHA, are important structural components of neuronal cell membranes.
They contribute to:
- Membrane fluidity
- Synaptic signaling
- Neuroinflammatory regulation
- Normal brain function
Several meta-analyses suggest that omega-3 supplementation—particularly formulations higher in EPA—may provide modest benefit for some individuals with depressive symptoms.
Although omega-3s are not a substitute for evidence-based mental health treatment, adequate intake through diet or supplementation when appropriate may support overall brain health.
Excellent dietary sources include:
- Salmon
- Sardines
- Mackerel
- Herring
- Trout
Nutrition Supports the Brain—It Does Not Replace Hormones
One of the most important messages women should understand is this:
Nutrition matters.
But nutrition alone cannot eliminate the hormonal fluctuations occurring during perimenopause.
Likewise, hormones alone cannot compensate for chronic sleep deprivation, inadequate protein intake, iron deficiency, uncontrolled diabetes, or persistent physiologic stress.
The healthiest approach recognizes that mood is influenced by multiple interconnected systems.
Hormones.
Sleep.
Nutrition.
Physical activity.
Stress physiology.
Metabolic health.
Mental health.
Each contributes to how resilient the brain is during the menopause transition.
Rather than searching for a single nutritional "miracle supplement," women often benefit most from building a strong physiologic foundation that supports overall brain function while addressing the hormonal changes occurring during midlife.
Clinical Pearl
Mood during perimenopause is influenced by far more than hormones alone.
Blood sugar instability, inadequate protein intake, iron deficiency, vitamin D deficiency, magnesium status, omega-3 intake, sleep, stress, and metabolic health can all affect brain function. While correcting these factors may not eliminate hormonal mood symptoms, optimizing overall health can improve the brain's resilience during the menopause transition and should be considered an important component of comprehensive care.
Stress During Midlife — When Hormonal Changes Meet Real Life
One of the greatest misconceptions about mood changes during perimenopause is that they are caused by hormones alone.
In reality, the menopause transition often occurs during one of the most demanding periods of a woman's life.
Many women in their 40s are simultaneously managing careers, raising children or teenagers, supporting aging parents, maintaining relationships, caring for their own health, and navigating increasing financial responsibilities.
These life demands occur at precisely the same time that the brain is adapting to fluctuating ovarian hormones.
The result is not simply "more stress."
It is the convergence of biologic vulnerability and increasing environmental demands.
Understanding this interaction helps explain why many women feel emotionally overwhelmed during midlife—even when they have successfully managed stress throughout much of their adult lives.
Midlife Is Often the Busiest Decade of Life
Unlike adolescence or early adulthood, midlife rarely involves only one major responsibility.
Instead, responsibilities tend to accumulate.
Many women are simultaneously balancing:
- Full-time careers
- Leadership roles
- Running businesses
- Raising young children
- Parenting teenagers
- Supporting children leaving home
- Caring for aging parents
- Managing chronic health conditions
- Financial responsibilities
- Marriage or relationship challenges
- Household management
- Community or religious commitments
Researchers sometimes describe this stage as the "sandwich generation," where women provide care for both younger and older generations at the same time.
Each responsibility requires emotional energy, attention, planning, and decision-making.
Collectively, these demands increase cognitive and emotional workload long before hormones enter the picture.
Hormonal Changes Reduce the Brain's Stress Resilience
Stress itself is not new.
What changes during perimenopause is often the brain's ability to adapt to stress.
Throughout the reproductive years, estrogen influences numerous brain systems involved in emotional regulation, stress adaptation, and cognitive flexibility.
As estrogen begins fluctuating unpredictably during perimenopause, these adaptive mechanisms become less stable.
Research suggests estrogen interacts with several regions involved in stress processing, including the:
- Prefrontal cortex
- Amygdala
- Hippocampus
- Hypothalamus
These regions help regulate:
- Emotional responses
- Executive function
- Memory
- Fear processing
- Stress recovery
When hormonal signaling becomes more variable, the same stressful event that once felt manageable may now feel significantly more overwhelming.
This does not mean women become weaker.
Rather, the brain is working under different physiologic conditions.
The Stress Response System
The body's primary stress response is coordinated through the hypothalamic-pituitary-adrenal (HPA) axis.
When the brain perceives stress, it initiates a cascade of hormonal signals that ultimately increase cortisol production by the adrenal glands.
In the short term, cortisol is adaptive.
It helps:
- Increase energy availability
- Maintain blood pressure
- Mobilize glucose
- Improve immediate survival during acute stress
However, chronic activation of the stress response may contribute to:
- Sleep disruption
- Anxiety
- Fatigue
- Impaired concentration
- Mood disturbances
- Increased emotional reactivity
Perimenopause does not necessarily cause abnormal cortisol production in every woman.
However, fluctuating ovarian hormones may alter how the brain perceives and responds to stress, making chronic life stress feel more difficult to manage.
Why Small Stressors Suddenly Feel Bigger
Many women describe an experience that sounds remarkably similar:
"I know this shouldn't upset me this much."
The situation itself may be relatively minor.
A child forgetting homework.
An unexpected work email.
Traffic.
A disagreement with a spouse.
A sink full of dishes.
Under ordinary circumstances, these events might have caused only mild frustration.
During perimenopause, however, the brain's ability to regulate emotional responses may become less efficient.
Instead of calmly processing the situation, emotional reactions may become:
- Faster
- More intense
- Longer-lasting
- Harder to regulate
This is not a character flaw.
It reflects the interaction between hormonal variability and cumulative stress.
Chronic Stress and Cognitive Load
Stress is not only emotional.
It is also cognitive.
Every responsibility requires the brain to process information, make decisions, solve problems, and switch attention between competing priorities.
Psychologists refer to this as cognitive load—the total amount of mental effort required at a given time.
Midlife women often carry an extraordinary cognitive workload that may include remembering:
- Children's schedules
- Medical appointments
- Medication refills
- Household tasks
- Work deadlines
- Financial obligations
- Family birthdays
- School activities
- Meal planning
- Aging parents' healthcare needs
Even when these tasks appear small individually, together they create continuous demands on executive function.
When hormonal fluctuations, poor sleep, and chronic stress are added to an already overloaded cognitive system, emotional resilience naturally declines.
Why Mood Symptoms Often Cluster Together
One of the hallmarks of perimenopause is that symptoms rarely occur in isolation.
A woman experiencing increased irritability may also notice:
- Brain fog
- Difficulty concentrating
- Anxiety
- Sleep disruption
- Fatigue
- Reduced patience
- Forgetfulness
- Feeling emotionally overwhelmed
These symptoms frequently occur together because many share common biologic pathways involving estrogen, sleep, neurotransmitters, stress physiology, and brain network function.
Rather than representing separate problems, they often reflect different manifestations of the same underlying physiologic transition.
Stress Management Is Not About Eliminating Stress
Many women become frustrated when they are told to simply "reduce stress."
For someone balancing work, caregiving, parenting, finances, and relationships, eliminating stress is rarely realistic.
The goal is not to create a stress-free life.
The goal is to improve the brain's capacity to recover from stress.
Evidence-based approaches that may improve stress resilience include:
- Regular physical activity
- Resistance training
- Consistent sleep schedules
- Mindfulness-based stress reduction
- Cognitive behavioral therapy (CBT)
- Social connection
- Time in nature
- Relaxation techniques
- Appropriate treatment of menopausal symptoms
- Addressing anxiety or depression when present
Small improvements in stress recovery can meaningfully improve emotional well-being over time.
The Bigger Picture
Perimenopause does not occur in a vacuum.
It unfolds during one of the busiest and most demanding chapters of a woman's life.
Hormonal fluctuations influence the brain's ability to regulate mood, but they do so within the broader context of careers, caregiving, relationships, financial pressures, sleep disruption, and accumulated cognitive load.
Understanding this interaction helps move the conversation away from blame.
Women are not "overreacting."
Nor are they simply "too emotional."
In many cases, they are navigating one of the most complex intersections of biology, psychology, and life circumstance that occurs across the female lifespan.
Recognizing this complexity is essential to providing compassionate, evidence-based care.
Clinical Pearl
Perimenopause does not make life more stressful—it often makes an already stressful life harder for the brain to navigate.
Mood changes during midlife are best understood through a biopsychosocial lens, where fluctuating hormones interact with chronic stress, sleep disruption, cognitive load, and life circumstances. Effective management often requires addressing both the biology of the menopause transition and the realities of women's daily lives.
Is It Perimenopause, PMS, PMDD, Anxiety, or Depression?
One of the greatest challenges in caring for women during midlife is that many conditions can produce similar emotional symptoms.
Irritability.
Anxiety.
Anger.
Mood swings.
Difficulty concentrating.
Fatigue.
Poor sleep.
Feeling emotionally overwhelmed.
These symptoms are common during perimenopause—but they are not unique to perimenopause.
This is one reason why an accurate evaluation is so important.
While hormonal fluctuations can certainly contribute to mood changes, other conditions such as premenstrual syndrome (PMS), premenstrual dysphoric disorder (PMDD), major depressive disorder, generalized anxiety disorder (GAD), thyroid disease, iron deficiency, medication effects, and other medical conditions may present with similar symptoms.
The goal is not to immediately assume that every emotional symptom is hormonal.
The goal is to understand the overall clinical picture.
A careful history remains one of the most valuable diagnostic tools.
Why Timing Matters
One of the most important clues is when symptoms occur.
Hormone-related mood symptoms often follow recognizable patterns.
Mental health disorders generally do not.
Understanding the timing of symptoms frequently provides valuable insight into the underlying cause.
For example:
A woman who feels emotionally well for most of the month but develops severe irritability five days before menstruation may have a very different diagnosis from a woman who experiences persistent depression every day for several months.
Although overlap certainly exists, symptom timing often guides further evaluation.
Comparing Common Causes of Mood Symptoms
| Feature | PMS | PMDD | Perimenopause | Major Depression | Generalized Anxiety Disorder |
|---------|-----|------|----------------|------------------|------------------------------|
| Typical age | Reproductive years | Reproductive years | Usually late 30s–50s | Any age | Any age |
| Timing | During the luteal phase before menstruation | During the luteal phase before menstruation | May fluctuate throughout the cycle or become less predictable as cycles become irregular | Persistent | Persistent |
| Relationship to menstrual cycle | Strong | Very strong | Variable | Usually none | Usually none |
| Symptoms improve after menstruation? | Yes | Yes | Sometimes, but patterns become less predictable | No | No |
| Common symptoms | Mild irritability, bloating, breast tenderness | Severe mood changes, anger, depression, marked irritability | Mood swings, anxiety, irritability, brain fog, sleep disturbance, hot flashes, irregular periods | Persistent sadness, loss of interest, fatigue, hopelessness | Excessive worry, restlessness, muscle tension, difficulty relaxing |
| Severity | Mild to moderate | Severe and functionally impairing | Mild to severe | Moderate to severe | Mild to severe |
| Effect on daily functioning | Usually limited | Significant impairment | Variable | Often significant | Often significant |
Premenstrual Syndrome (PMS)
PMS affects many women during their reproductive years.
Symptoms typically develop during the late luteal phase—the days before menstruation—and improve shortly after the menstrual period begins.
Common symptoms include:
- Irritability
- Mood changes
- Breast tenderness
- Bloating
- Food cravings
- Fatigue
- Mild anxiety
Although PMS can certainly be uncomfortable, symptoms generally do not cause severe impairment in daily functioning.
Premenstrual Dysphoric Disorder (PMDD)
PMDD is much more than "bad PMS."
It is a recognized medical disorder characterized by severe mood symptoms that occur during the luteal phase of the menstrual cycle.
Women with PMDD may experience:
- Intense anger
- Marked irritability
- Severe anxiety
- Depression
- Emotional lability
- Feelings of hopelessness
- Difficulty functioning at work or home
Symptoms typically improve within several days after menstruation begins.
PMDD affects a relatively small percentage of menstruating women but can have a profound impact on quality of life.
Importantly, PMDD should not be dismissed as simply "being emotional."
Evidence-based treatments are available.
Perimenopause
Perimenopause differs from both PMS and PMDD because hormone production becomes increasingly unpredictable.
Rather than experiencing symptoms at exactly the same point each month, women may notice:
- Mood changes occurring earlier or later than expected
- Symptoms that vary from cycle to cycle
- Increasing irregularity of menstrual periods
- Hot flashes
- Night sweats
- Sleep disturbance
- Brain fog
- Reduced stress tolerance
Some women continue to experience symptoms primarily before menstruation.
Others notice mood changes throughout increasingly irregular cycles.
Because hormonal fluctuations become less predictable, symptom patterns often become less predictable as well.
Major Depressive Disorder
Depression is more than feeling sad.
It is a medical condition that affects mood, thinking, behavior, sleep, appetite, and energy.
Symptoms may include:
- Persistent sadness
- Loss of interest or pleasure
- Fatigue
- Feelings of worthlessness
- Difficulty concentrating
- Changes in appetite
- Sleep disturbance
- Thoughts of death or suicide
Unlike hormone-related mood symptoms, depression is generally not limited to one phase of the menstrual cycle.
Symptoms are usually present most days for at least two weeks and often persist much longer without treatment.
Perimenopause can increase vulnerability to depression in some women, particularly those with a previous history of depressive disorders.
This is one reason careful evaluation is essential.
Generalized Anxiety Disorder (GAD)
Many women experience increased anxiety during perimenopause.
However, not every woman with anxiety has generalized anxiety disorder.
GAD is characterized by excessive, persistent worry that is difficult to control and occurs across multiple aspects of daily life.
Women with GAD often experience:
- Constant worry
- Restlessness
- Feeling "on edge"
- Muscle tension
- Difficulty relaxing
- Trouble concentrating
- Poor sleep
Like depression, generalized anxiety disorder is not usually linked to menstrual cycle timing.
Hormonal fluctuations may worsen underlying anxiety, but they are rarely the only explanation.
More Than One Condition Can Exist Together
One of the most important concepts in women's mental health is that these diagnoses are not mutually exclusive.
A woman may experience:
- Perimenopause and depression.
- Perimenopause and generalized anxiety disorder.
- Perimenopause and PMDD.
- Perimenopause complicated by chronic stress and sleep deprivation.
Hormonal fluctuations may increase vulnerability to emotional symptoms while pre-existing psychiatric conditions continue to influence overall mental health.
This is why individualized assessment remains so important.
When Should You Seek Medical Evaluation?
Although mood changes are common during perimenopause, they should never be dismissed when they become severe or persistent.
You should speak with your healthcare professional if:
- Anger is affecting your relationships.
- Mood symptoms interfere with work or daily functioning.
- You experience severe anxiety or panic attacks.
- Symptoms occur most days rather than only around your menstrual cycle.
- Sleep disruption becomes persistent.
- You lose interest in activities you normally enjoy.
- You experience feelings of hopelessness.
- You have thoughts of self-harm or suicide.
Suicidal thoughts should always be treated as a medical emergency requiring immediate evaluation.
Why a Comprehensive Evaluation Matters
There is no single blood test that can diagnose perimenopausal mood changes.
Diagnosis depends on understanding the whole clinical picture, including:
- Age
- Menstrual history
- Symptom timing
- Sleep quality
- Vasomotor symptoms
- Medical history
- Medication use
- Mental health history
- Life stressors
- Physical examination when appropriate
- Laboratory evaluation when clinically indicated
This comprehensive approach allows clinicians to distinguish hormonal changes from other medical and psychiatric conditions while developing an individualized treatment plan.
Clinical Pearl
Not every mood change during midlife is caused by perimenopause—but neither should hormonal changes be overlooked.
The timing, pattern, severity, and duration of symptoms provide valuable diagnostic clues. A thoughtful clinical evaluation helps distinguish perimenopause from PMS, PMDD, depression, generalized anxiety disorder, and other medical conditions, ensuring women receive appropriate, evidence-based care.
Evidence-Based Strategies That May Help
One of the most important messages women should hear is this:
You do not have to simply "live with" severe mood changes during perimenopause.
Although emotional symptoms are common during the menopause transition, there are evidence-based lifestyle strategies and medical treatments that may improve quality of life for many women.
The most effective approach is rarely a single intervention.
Instead, mood is often best supported by addressing multiple contributors simultaneously, including hormonal changes, sleep, physical activity, nutrition, stress physiology, and underlying mental health conditions when present.
Treatment should always be individualized.
Every woman's medical history, symptom severity, risk factors, personal preferences, and treatment goals are different.
Lifestyle Strategies That Support Emotional Well-Being
Lifestyle interventions should not be viewed as a replacement for appropriate medical care.
However, they form the foundation of healthy aging and may significantly improve emotional resilience during the menopause transition.
Regular Physical Activity
Exercise is one of the most consistently supported lifestyle interventions for overall health during midlife.
Regular physical activity has been associated with improvements in:
- Mood
- Anxiety symptoms
- Sleep quality
- Energy levels
- Cardiovascular health
- Insulin sensitivity
- Cognitive function
- Overall quality of life
Exercise also promotes the release of endorphins while supporting long-term brain health through improved cerebral blood flow and neuroplasticity.
The goal is not perfection.
The goal is consistency.
Strength Training
If there is one form of exercise that deserves particular attention during perimenopause, it is resistance training.
Strength training supports much more than muscle mass.
It contributes to:
- Improved insulin sensitivity
- Better glucose regulation
- Increased bone strength
- Preservation of lean body mass
- Improved physical function
- Better metabolic health
- Greater confidence and self-efficacy
Emerging evidence also suggests resistance exercise may positively influence mood and anxiety symptoms while improving resilience to stress.
As discussed in our article "Muscle Is a Midlife Organ," maintaining skeletal muscle is one of the most important investments women can make for healthy aging.
Prioritize Sleep
Because sleep and emotional regulation are closely connected, improving sleep should be considered a central component of mood management.
Strategies may include:
- Maintaining a consistent sleep schedule
- Limiting caffeine late in the day
- Creating a cool, dark sleep environment
- Reducing evening screen exposure
- Addressing hot flashes or night sweats
- Evaluating persistent insomnia with a healthcare professional
Improving sleep often improves far more than fatigue.
Many women also notice improvements in patience, concentration, emotional resilience, and stress tolerance.
A Mediterranean-Style Eating Pattern
Nutrition influences multiple physiologic systems involved in brain health.
Although no single diet eliminates perimenopausal symptoms, a Mediterranean-style eating pattern has consistently been associated with improved cardiovascular and metabolic health.
This dietary pattern emphasizes:
- Vegetables
- Fruits
- Whole grains
- Legumes
- Nuts
- Olive oil
- Fish
- Lean protein sources
It also limits:
- Ultra-processed foods
- Refined sugars
- Excess saturated fats
Combined with adequate protein intake, this approach supports healthy aging while helping maintain stable energy and metabolic health.
Stress Reduction
Stress cannot always be eliminated.
But improving recovery from stress is often possible.
Evidence-based approaches include:
- Mindfulness meditation
- Deep breathing exercises
- Yoga
- Time in nature
- Regular physical activity
- Prayer or spiritual practices
- Journaling
- Maintaining meaningful social connections
The goal is not to remove every source of stress.
The goal is to improve the brain's ability to recover from it.
Alcohol
Many women notice that alcohol affects them differently during perimenopause.
Alcohol may contribute to:
- Poor sleep
- Increased anxiety
- Mood changes
- Night sweats
- Hot flashes
Reducing alcohol intake may improve both sleep quality and emotional well-being for some women.
Smoking Cessation
Smoking has been associated with earlier menopause and increased cardiovascular risk.
It may also worsen vasomotor symptoms and negatively affect overall health.
For women who smoke, cessation remains one of the most important interventions for long-term health.
Mindfulness and Emotional Awareness
Mindfulness is not about eliminating emotions.
It is about changing our relationship with them.
Research suggests mindfulness-based interventions may improve:
- Stress management
- Anxiety
- Emotional regulation
- Sleep quality
- Overall well-being
For many women, learning to observe emotions without immediately reacting to them becomes an important skill during the menopause transition.
Medical Treatments That May Help
Lifestyle interventions are important.
However, some women experience symptoms that significantly affect daily functioning despite healthy habits.
Medical treatment should be considered when symptoms are moderate to severe or interfere with quality of life.
Menopausal Hormone Therapy (MHT)
For appropriately selected women, menopausal hormone therapy (MHT) is considered the most effective treatment for bothersome vasomotor symptoms such as hot flashes and night sweats.
By improving vasomotor symptoms and sleep quality, MHT may also improve overall quality of life and emotional well-being in some women.
For women with mood symptoms occurring alongside significant vasomotor symptoms, MHT may be considered when clinically appropriate after an individualized discussion of potential benefits and risks.
MHT is not appropriate for every woman.
Treatment decisions should consider:
- Age
- Time since menopause
- Personal medical history
- Family history
- Cardiovascular risk
- Breast cancer risk
- Individual treatment goals
Shared decision-making remains essential.
Antidepressant Medications (SSRIs and SNRIs)
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) have strong evidence supporting their use in treating depression and anxiety disorders.
Certain SSRIs and SNRIs have also demonstrated benefit in reducing vasomotor symptoms in some women.
These medications may be particularly helpful when:
- Depression is present
- Anxiety is significant
- Hormone therapy is not appropriate
- Vasomotor symptoms coexist with mood symptoms
Medication selection should always be individualized.
Cognitive Behavioral Therapy (CBT)
Cognitive Behavioral Therapy (CBT) is one of the most extensively studied psychological treatments for mood disorders.
CBT helps individuals identify and modify patterns of thinking and behavior that contribute to emotional distress.
Research suggests CBT may improve:
- Anxiety
- Depression
- Insomnia
- Stress management
- Coping with menopausal symptoms
Importantly, CBT does not imply that symptoms are "all in your head."
Rather, it provides practical tools that help the brain respond differently to stress.
Individualized Treatment Options
Every woman's experience is unique.
Depending on the clinical situation, treatment may also include:
- Management of iron deficiency or other nutritional deficiencies
- Treatment of thyroid disease or other underlying medical conditions
- Evaluation and treatment of sleep disorders
- Referral to a mental health professional when appropriate
- Management of chronic pain or other contributing conditions
Successful treatment often requires addressing multiple contributing factors rather than focusing on hormones alone.
Shared Decision-Making Matters
There is no single "best" treatment for every woman.
The most appropriate management plan depends on:
- Symptom severity
- Medical history
- Personal preferences
- Treatment goals
- Risk factors
- Lifestyle
- Family history
Some women improve significantly with lifestyle changes.
Others benefit from hormone therapy.
Some require treatment for depression or anxiety.
Many benefit from a combination of approaches.
The goal is not simply to reduce symptoms.
The goal is to improve overall health, emotional well-being, and quality of life throughout the menopause transition.
Working with a qualified healthcare professional allows women to weigh the potential benefits and risks of each option while developing a treatment plan that reflects their individual needs and values.
Clinical Pearl
Perimenopause mood changes are treatable.
The strongest evidence supports a comprehensive approach that combines healthy lifestyle habits, optimized sleep, regular physical activity, stress management, and individualized medical care when appropriate.
Rather than searching for a single solution, women often achieve the greatest improvement by addressing the multiple biologic and lifestyle factors that influence emotional well-being during the menopause transition.
When Should You Talk With Your Healthcare Professional?
Although mood changes are common during perimenopause, they should never be dismissed simply because they occur during midlife.
Experiencing increased irritability, frustration, or emotional sensitivity does not mean that women should simply "learn to live with it."
One of the most important advances in menopause medicine over the past two decades has been the recognition that emotional symptoms deserve the same thoughtful evaluation as physical symptoms.
Just as persistent chest pain warrants medical attention, significant changes in emotional health also deserve careful assessment.
Seeking medical care is not a sign of weakness.
It is an important step toward understanding what is happening, identifying contributing factors, and developing an individualized treatment plan.
When Should You Seek Medical Evaluation?
You should consider scheduling an appointment with your healthcare professional if your symptoms:
- Interfere with your ability to perform at work.
- Affect your relationships with your partner, family, friends, or coworkers.
- Cause frequent conflict or emotional distress.
- Prevent you from enjoying activities you normally enjoy.
- Persist beyond the days surrounding your menstrual cycle.
- Become progressively worse over time.
- Are accompanied by severe anxiety or panic attacks.
- Include persistent sadness or feelings of hopelessness.
- Are associated with significant sleep disruption or overwhelming fatigue.
- Represent a sudden or dramatic change from your usual personality or emotional functioning.
These symptoms may still be related to perimenopause—but they also deserve evaluation to exclude other medical or psychiatric conditions that may require treatment.
When Symptoms Require Immediate Attention
Some emotional symptoms should never be ignored.
Seek immediate medical attention if you experience:
- Thoughts of self-harm or suicide.
- Thoughts of harming someone else.
- Severe depression that interferes with basic daily functioning.
- Panic attacks that are becoming increasingly frequent or disabling.
- New confusion, hallucinations, or other significant changes in thinking or behavior.
These situations require prompt evaluation and should not be attributed to hormones alone.
If you are experiencing thoughts of suicide or believe you may be in immediate danger, call your local emergency services or go to the nearest emergency department immediately.
A Comprehensive Evaluation Matters
There is no single blood test that can diagnose mood changes caused by perimenopause.
Instead, healthcare professionals evaluate the entire clinical picture.
This may include:
- Your age and menstrual history.
- The timing of your symptoms.
- Sleep quality.
- Vasomotor symptoms such as hot flashes and night sweats.
- Current medications.
- Medical and psychiatric history.
- Family history.
- Lifestyle factors.
- Physical examination when appropriate.
- Laboratory testing when clinically indicated to evaluate for contributing conditions such as thyroid disease, iron deficiency, or other medical disorders.
Because emotional symptoms often result from multiple interacting factors, a comprehensive evaluation is far more valuable than focusing on hormones alone.
You Do Not Have to Navigate This Alone
Many women spend months—or even years—wondering why they feel so different.
Some blame themselves.
Others worry they are becoming impatient, difficult, or emotionally unstable.
Many never realize that the menopause transition may be contributing to what they are experiencing.
The good news is that understanding has advanced tremendously.
Healthcare professionals now recognize that the menopause transition affects far more than the reproductive system.
It also influences the brain, sleep, metabolism, cardiovascular health, bone, muscle, and emotional well-being.
Most importantly, effective support is available.
Whether your symptoms are primarily related to hormonal fluctuations, sleep disruption, chronic stress, depression, anxiety, or a combination of these factors, you deserve compassionate, evidence-based care.
Seeking help is not giving up.
It is taking an important step toward protecting your long-term health and quality of life.
Key Takeaways
The menopause transition is one of the most significant biologic transitions in a woman's life.
Understanding the science behind these changes can replace fear, confusion, and self-blame with knowledge and confidence.
The most important messages to remember are:
- Anger, irritability, and emotional sensitivity are common symptoms during perimenopause. Many women experience noticeable mood changes as hormone production becomes increasingly unpredictable.
- Hormonal fluctuations influence the brain. Estrogen and progesterone affect neurotransmitters involved in mood, emotional regulation, sleep, cognition, and stress resilience. During perimenopause, fluctuating hormone levels—not simply low hormone levels—can contribute to emotional symptoms.
- Mood is influenced by multiple interconnected factors. Sleep quality, chronic stress, nutrition, blood sugar regulation, metabolic health, physical activity, and underlying medical or mental health conditions all interact with hormonal changes to shape emotional well-being.
- Effective treatment options are available. Lifestyle strategies, cognitive behavioral therapy, menopausal hormone therapy for appropriately selected women, antidepressant medications when indicated, and individualized medical care can all play important roles in improving quality of life.
- You are not "losing yourself." Your body—and your brain—are adapting to a complex neuroendocrine transition. Understanding what is happening allows you to seek appropriate support and make informed decisions about your health.
Perhaps the most important message is this:
Perimenopause is not simply a reproductive transition.
It is also a brain transition.
The emotional changes many women experience are not a reflection of personal weakness or failure.
They are part of a complex interaction between hormones, brain physiology, sleep, stress, metabolism, and the realities of midlife.
With greater understanding, evidence-based care, and compassionate support, women can navigate this transition with confidence.
Because the goal is not merely to survive perimenopause.
It is to protect your emotional health, your brain health, and your quality of life for the decades that follow.
Evidence Base
This article is informed by current evidence from leading professional organizations and peer-reviewed scientific literature on the menopause transition, women's mental health, neuroendocrinology, and healthy aging.
Key references include:
- The Menopause Society (formerly the North American Menopause Society). Evidence-based position statements and clinical guidance on the management of menopause, vasomotor symptoms, mood changes, menopausal hormone therapy, and healthy aging.
- International Menopause Society (IMS). Global recommendations and expert consensus statements on menopause management, women's health, and quality of life during the menopause transition.
- American College of Obstetricians and Gynecologists (ACOG). Clinical guidance on perimenopause, menopause, mood disorders, and comprehensive midlife care.
- National Institute for Health and Care Excellence (NICE). Menopause: Diagnosis and Management (NG23). Evidence-based recommendations for the assessment and management of menopause-related symptoms, including psychological symptoms.
- The Endocrine Society. Clinical practice guidelines relevant to endocrine health, hormone physiology, metabolic health, and selected aspects of menopause care where applicable.
- Study of Women's Health Across the Nation (SWAN). A landmark longitudinal study that has significantly advanced our understanding of hormonal changes, mood symptoms, sleep, cognition, cardiovascular health, and healthy aging throughout the menopause transition.
- Peer-reviewed scientific literature examining:
- Estrogen and brain physiology
- Progesterone and neurosteroids (including allopregnanolone)
- Serotonin, dopamine, GABA, glutamate, and norepinephrine
- Emotional regulation during perimenopause
- Sleep and emotional processing
- Stress physiology and the hypothalamic-pituitary-adrenal (HPA) axis
- Nutrition, metabolic health, and mood
- Menopausal hormone therapy
- Cognitive behavioral therapy
- Depression, anxiety, PMDD, and women's mental health during the menopause transition
Because research continues to evolve, recommendations may change as new evidence becomes available. Women experiencing significant mood changes should discuss their symptoms with a qualified healthcare professional to determine the most appropriate evaluation and individualized treatment plan.
Related Articles
Continue learning about the menopause transition:
- Why Am I Waking Up at 3 AM During Perimenopause?
- Muscle Is a Midlife Organ: Why Strength Training Is Medicine During Perimenopause
- Magnesium and Perimenopause: What the Evidence Says
- Intermittent Fasting During Perimenopause: Benefits, Risks, and What Women Should Know
- Perimenopause Weight Gain: Why It Happens and What the Science Says
- Heart Palpitations During Perimenopause: Understanding the Connection
Medical Disclaimer: This article is intended for educational purposes only and should not be considered a substitute for individualized medical advice, diagnosis, or treatment. Always consult a qualified healthcare professional regarding your personal medical concerns.